A needs assessment in care sits at the very heart of person-centred care. Without it, care plans are guesswork, support packages are misaligned, and individuals risk receiving services that do not reflect their actual situation, preferences, or level of risk.
The pressure on assessors, care coordinators, and registered managers to get this right has never been greater. Local authority funding decisions, CQC compliance, and above all, the dignity and safety of service users all depend on the quality of assessment that takes place before a single hour of support is delivered.
A situation that comes up regularly in care management training reflects exactly where the anxiety tends to sit:
"There is nothing worse than reading a care plan that’s months out of date. It’s like reading a biography of a stranger while the actual person is right there, waiting for you to notice them. We owe it to them to get the story right from day one."
Whether you are a newly qualified care coordinator, an experienced social worker, or a registered manager reviewing your team’s assessment practice, this guide will walk you through the seven steps to conducting a successful needs assessment in care from first contact through to finalising the plan and preparing for review.

What Is a Needs Assessment in Care?
A needs assessment in care is a structured process through which a trained professional evaluates an individual’s care and support needs in relation to their physical, mental, emotional, and social well-being.
The Care Act 2014 requires that assessments consider the individual’s well-being holistically and focus on outcomes rather than tasks. The well-being principle must underpin every stage of the assessment, ensuring the process respects the person’s dignity, independence, and right to make informed decisions. The assessment must consider:
• What the person can do for themselves
• What they need support with
• What outcomes matter most to them
• What strengths, assets, and informal support networks do they have available
Local authorities are to consider how to involve an individual in their assessment in the way most appropriate to them. This may include using communication aids, a preferred language, or an independent advocate where the person has substantial difficulty participating.
Why a Needs Assessment Matters in Care
Under the Care Act 2014, every adult who appears to have care and support needs has the right to a needs assessment, regardless of their financial position or the likelihood that the local authority will fund their care. This is a statutory entitlement, not a discretionary decision.
A properly conducted needs assessment in care:
• Establishes a clear, evidence-based picture of an individual’s strengths, needs, risks, and outcomes
• Ensures the care plan that follows is genuinely person-centred and proportionate
• Provides a defensible record if decisions are challenged by the individual, their family, or a regulator
• Supports the allocation of appropriate and cost-effective resources
CQC inspectors regularly scrutinise assessment documentation when evaluating whether a service is Responsive and Safe. Incomplete or generic assessments are a consistent source of regulatory concern.

Steps to Conducting a Successful Needs Assessment
Step 1: Prepare Before the Assessment
Before the assessment meeting takes place, gather as much relevant background information as possible. This includes any previous:
● Care assessments or reviews
● Medical records or GP correspondence where consent has been given
● information from referrers, family members, or other professionals involved in the person’s care, and details of any existing formal or informal support in place.
Note: Preparation prevents duplication and demonstrates respect for the individual’s time and dignity.
Step 2: Build Rapport and Explain the Purpose
The opening of a needs assessment in care is not administrative. It is relational. The way the assessment begins will shape the quality of information shared throughout.
Introduce yourself clearly and explain the purpose of the assessment, how the information gathered will be used, the person’s right to be accompanied by a family member, carer, or advocate, and the fact that the assessment is confidential within the limits of safeguarding obligations.
People share more, and more accurately, when they feel safe, respected, and genuinely listened to.
Step 3: Assess Needs Holistically
A good needs assessment in care looks beyond the presenting issue. Using a structured tool such as the Outcomes Star, the Resource Allocation System (RAS), or your local authority’s approved framework, explore the following domains:
• Physical health and medical needs
• Mental health, emotional well-being, and cognitive functioning
• Ability to maintain personal hygiene and manage daily living activities
• Nutrition and hydration
• Housing and immediate environment
• Social connections and risk of isolation
• Safety and safeguarding considerations
• Informal support from family, friends, or community networks
Do not limit the conversation to what the person cannot do. The Care Act 2014 places a statutory duty on assessors to identify and build on existing strengths and assets.
Step 4: Identify Eligible Needs and Outcomes
Once the full picture has been gathered, the assessor must determine which of the identified needs meet the eligibility criteria under the Care Act 2014. In England, the national minimum eligibility threshold is set out in the Care and Support (Eligibility Criteria) Regulations 2015.
A need is eligible where it arises from a physical or mental impairment or illness, the person is unable to achieve two or more specified outcomes as a result, and there is or is likely to be a significant impact on the person’s wellbeing.
Eligible needs trigger a legal duty on the local authority to meet those needs. Document the eligibility decision clearly and with reasoning.
Step 5: Involve the Individual in Care Planning
The needs assessment does not produce a care plan in isolation. The assessment findings must be shared with the individual and used as the basis for a collaborative conversation about how their needs will be met.
Person-centred care planning requires that the individual’s voice shapes the outcome, not just informs it. Ask the individual what outcomes matter most to them, how they would like support to be delivered, any particular preferences, and who else they would like involved.
Step 6: Document the Assessment Accurately and Promptly
Documentation is not secondary to assessment. It is an integral part of it. Your written record must accurately reflect what was said and observed, use objective and factual language rather than interpretation or assumption, clearly separate the person’s own words from the assessor’s professional judgement, be completed promptly, ideally on the same day or within 24 hours and be shared with the individual and, where appropriate, their representative.
Never record information you did not gather, and never omit information that may affect risk or eligibility decisions. Both have regulatory and potentially legal consequences.
Step 7: Set a Review Date and Monitor
A needs assessment in care is not a one-time event. The Care Act 2014 places a duty on local authorities to review care and support plans at least once in the first year following the assessment, and subsequently at appropriate intervals.
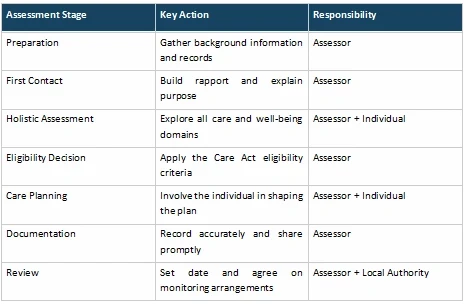
At the point of completing the assessment, agree on a clear review date with the individual, identify any triggers for an earlier review, and ensure all parties know who holds the lead responsibility for requesting a review. The table below gives an overview of the process:
Elevate Your Needs Assessment Practice
The quality of a needs assessment in care determines the quality of everything that follows. A thorough, honest, and person-centred assessment does more than just tick a box; it protects the individual and provides the foundation for care that genuinely improves lives
As Ruth Serena, a Senior Practitioner in Adult Social Care, puts it:
"Good care starts with a good conversation. The colleagues I admire most are the ones who refuse to rush the process. They treat the documentation with as much respect as the person they’re sitting with."
We know the pressure to complete paperwork quickly is real. But the evidence is clear: when we rush the assessment, we risk missing the person. Whether you are refining your approach or starting from scratch, remember that the documentation is the voice of the person you support.
Don't just fill in forms. Build a foundation for better care. But first, listen!
Transform Your Assessments Today!